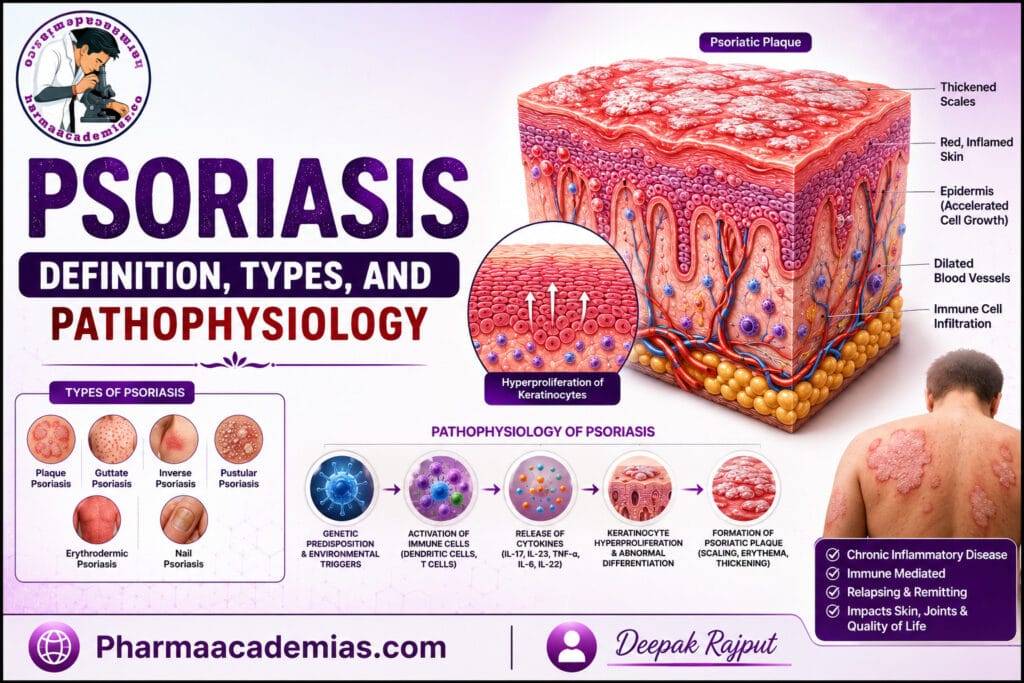
What is Psoriasis: Psoriasis is a chronic, immune-mediated, inflammatory skin disease characterized by excessive proliferation of skin cells, abnormal differentiation of keratinocytes, inflammation, and the formation of well-defined erythematous (red), scaly plaques. It is one of the most common chronic dermatological disorders, affecting approximately 2–3% of the global population, although its prevalence varies among different ethnic groups and geographic regions. Pharmaacademias.com
Psoriasis is not an infectious or contagious disease, meaning it cannot spread from one person to another through direct contact. Instead, it develops due to a complex interaction between genetic predisposition, immune system dysfunction, and environmental triggers. Individuals with psoriasis often experience repeated episodes of flare-ups and remissions throughout their lifetime.
The disease primarily affects the skin, but it is now recognized as a systemic inflammatory disorder because it may also involve the joints, nails, cardiovascular system, and other organs. Approximately 20–30% of patients with psoriasis eventually develop psoriatic arthritis, a chronic inflammatory joint disease that can lead to permanent joint damage if left untreated.
The hallmark feature of psoriasis is the rapid turnover of epidermal cells. Under normal conditions, skin cells require about 28–30 days to mature and reach the skin surface. In psoriasis, this process accelerates dramatically, taking only 3–5 days, leading to the accumulation of immature keratinocytes that form thick, silvery-white scales.
Definition of Psoriasis What is Psoriasis
Psoriasis is defined as a chronic autoimmune inflammatory skin disorder characterized by accelerated epidermal cell proliferation, abnormal keratinocyte differentiation, immune cell activation, and persistent inflammation, resulting in erythematous plaques covered with silvery-white scales.
The disease follows a chronic relapsing-remitting course and may significantly affect the patient’s physical, psychological, and social well-being.
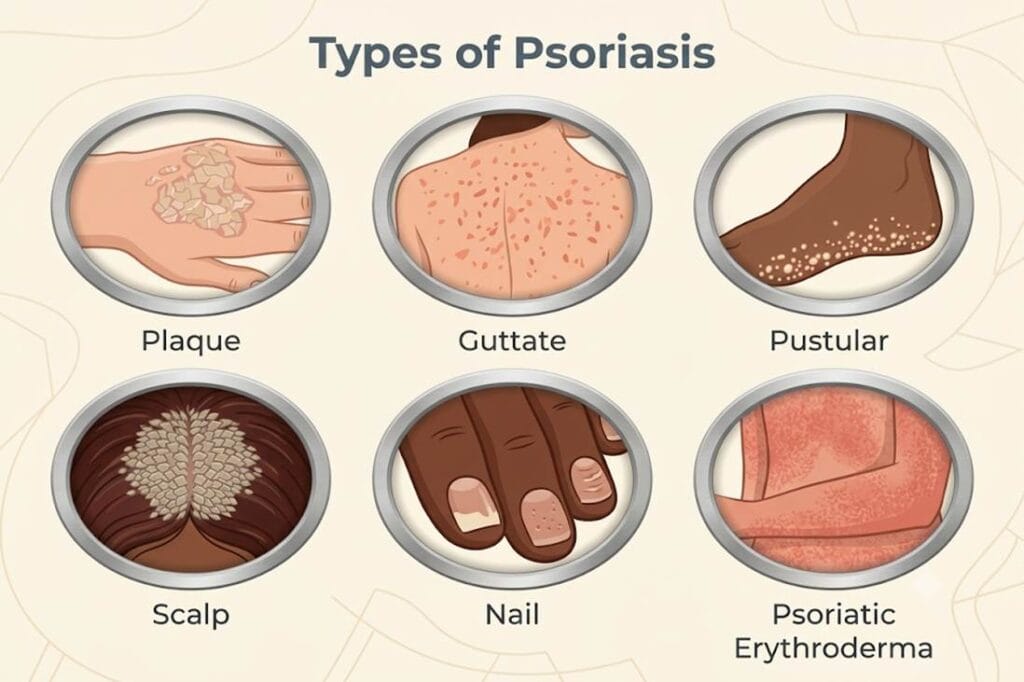
Types of Psoriasis
Although plaque psoriasis is the most common form, psoriasis exists in several clinical variants based on lesion morphology, distribution, and severity.
1. Plaque Psoriasis (Psoriasis Vulgaris)
Plaque psoriasis accounts for approximately 80–90% of all psoriasis cases, making it the most common type.
It presents as well-demarcated, raised, red plaques covered with thick, silvery-white scales. These plaques commonly appear on the elbows, knees, scalp, lower back, and extensor surfaces of the limbs. Patients often complain of itching, burning, or discomfort, although some lesions may remain asymptomatic.
2. Guttate Psoriasis
Guttate psoriasis is characterized by the sudden appearance of numerous small, drop-shaped lesions scattered over the trunk, arms, and legs.
It frequently develops after streptococcal throat infections, particularly in children and young adults. In some patients, guttate psoriasis resolves spontaneously, whereas others later develop chronic plaque psoriasis.
3. Inverse (Flexural) Psoriasis
Inverse psoriasis affects skin folds such as the:
- Armpits
- Groin
- Under the breasts
- Genital region
- Buttock cleft
Unlike plaque psoriasis, lesions are smooth, shiny, red, and usually lack thick scaling because friction and moisture prevent scale accumulation.
4. Pustular Psoriasis
Pustular psoriasis is characterized by sterile (non-infectious) pustules filled with white blood cells.
It may occur as:
- Localized pustular psoriasis (commonly affecting palms and soles)
- Generalized pustular psoriasis (rare but potentially life-threatening)
Generalized pustular psoriasis is associated with fever, chills, fatigue, leukocytosis, and systemic inflammation requiring urgent medical management.
5. Erythrodermic Psoriasis
This is the rarest but one of the most severe forms of psoriasis.
It involves widespread redness, inflammation, and scaling affecting more than 90% of the body’s surface area. Patients often develop severe dehydration, electrolyte imbalance, impaired temperature regulation, and increased risk of infection.
Erythrodermic psoriasis constitutes a dermatological emergency requiring hospitalization.
6. Nail Psoriasis
Nail involvement may occur alone or alongside skin lesions.
Common features include:
- Nail pitting
- Yellow-brown discoloration (“oil drop” sign)
- Nail thickening
- Separation of the nail from the nail bed (onycholysis)
- Crumbling nails
Nail psoriasis is strongly associated with psoriatic arthritis.
7. Psoriatic Arthritis
Psoriatic arthritis is an inflammatory joint disease occurring in patients with psoriasis.
Symptoms include:
- Joint pain
- Swelling
- Morning stiffness
- Reduced mobility
- Progressive joint destruction in severe cases
Early diagnosis and treatment are essential to prevent irreversible disability.
Pathophysiology of Psoriasis
The pathophysiology of psoriasis is complex and involves a continuous interaction between genetic susceptibility, environmental triggers, innate immunity, adaptive immunity, inflammatory cytokines, and abnormal keratinocyte proliferation. Modern research has shown that psoriasis is primarily an immune-mediated disease, with the skin changes occurring as a consequence of immune system dysregulation.
1. Genetic Predisposition
The development of psoriasis begins with an inherited genetic susceptibility. More than 80 genetic loci have been associated with psoriasis, with the strongest association found in the PSORS1 region on chromosome 6, particularly the HLA-Cw6 allele.
Individuals carrying these susceptibility genes are more likely to develop psoriasis when exposed to appropriate environmental triggers. However, genetic predisposition alone is insufficient; external factors are usually required to initiate disease.
2. Environmental Triggers
Several environmental factors can activate the immune system and precipitate psoriasis in genetically predisposed individuals.
Common triggers include:
- Streptococcal infections
- Skin injury (Koebner phenomenon)
- Psychological stress
- Cold weather
- Smoking
- Alcohol consumption
- Certain medications (lithium, beta-blockers, antimalarials)
- Obesity
- Hormonal changes
These triggers activate immune cells present in the skin.
3. Activation of Innate Immune System
Following skin injury or infection, damaged keratinocytes release antimicrobial peptides such as LL-37, DNA fragments, and inflammatory mediators.
These molecules activate dendritic cells, macrophages, neutrophils, and other innate immune cells.
Activated dendritic cells migrate to nearby lymph nodes where they present antigens to naïve T lymphocytes.
This marks the beginning of the adaptive immune response.
4. Activation of T Lymphocytes
Activated dendritic cells release cytokines such as:
- Interleukin-12 (IL-12)
- Interleukin-23 (IL-23)
These cytokines stimulate differentiation of naïve T cells into:
- Th1 cells
- Th17 cells
- Th22 cells
Among these, Th17 cells play the central role in psoriasis.
Activated T cells migrate back into the skin and release numerous inflammatory cytokines.
5. Cytokine Cascade (Central Mechanism)
The hallmark of psoriasis is an exaggerated cytokine network that perpetuates inflammation.
The most important cytokines include:
Tumor Necrosis Factor-alpha (TNF-α)
TNF-α is one of the earliest inflammatory mediators released by activated immune cells.
It promotes:
- Endothelial activation
- Recruitment of inflammatory cells
- Cytokine amplification
- Chronic inflammation
Because of its pivotal role, TNF-α is a major therapeutic target in psoriasis.
Interleukin-23 (IL-23)
IL-23 is produced primarily by activated dendritic cells.
Its major function is maintaining and expanding Th17 lymphocytes.
Without IL-23, the Th17 inflammatory pathway cannot be sustained.
Consequently, IL-23 inhibitors have become highly effective treatments for moderate-to-severe psoriasis.
Interleukin-17 (IL-17)
IL-17 is considered one of the most important cytokines responsible for psoriasis.
It stimulates keratinocytes to produce:
- Pro-inflammatory cytokines
- Chemokines
- Antimicrobial peptides
- Growth factors
This creates a self-perpetuating inflammatory cycle that continuously recruits immune cells into the skin.
Interleukin-22 (IL-22)
IL-22 directly stimulates keratinocyte proliferation while inhibiting their normal maturation.
As a result:
- Epidermis becomes markedly thickened.
- Skin cells remain immature.
- Thick plaques develop.
6. Hyperproliferation of Keratinocytes
Normally, keratinocytes require approximately 28–30 days to mature.
In psoriasis, inflammatory cytokines accelerate this process to only 3–5 days.
Because cells reach the surface before completing maturation:
- They retain nuclei.
- They fail to differentiate normally.
- Excessive keratin accumulates.
- Thick scales form.
This accelerated epidermal turnover explains the characteristic silvery-white plaques.
7. Angiogenesis
Inflammatory cytokines stimulate production of vascular endothelial growth factor (VEGF).
VEGF promotes formation of numerous new blood vessels within the dermis.
These dilated capillaries produce:
- Redness (erythema)
- Increased blood flow
- Easy bleeding after scale removal (Auspitz sign)
8. Chronic Inflammatory Feedback Loop
One of the most important features of psoriasis is the presence of a positive feedback cycle.
The sequence is as follows:
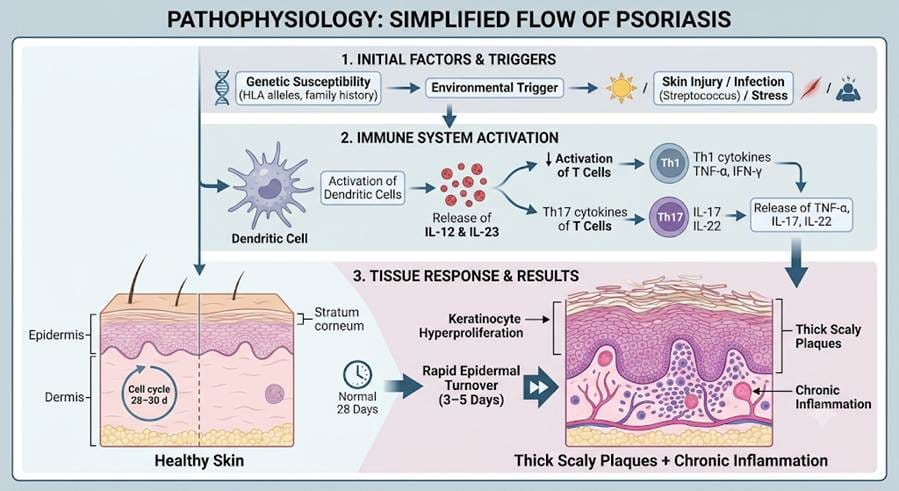
Skin injury or infection activates dendritic cells, which release IL-23 and IL-12. These cytokines activate Th17 and Th1 lymphocytes. Activated T cells produce IL-17, IL-22, TNF-α, IFN-γ, and other inflammatory mediators. These cytokines stimulate keratinocytes to proliferate rapidly and produce additional inflammatory cytokines and chemokines. The newly released mediators recruit more immune cells into the skin, resulting in persistent inflammation and continued plaque formation.
Because this cycle continuously reinforces itself, psoriasis becomes a chronic disease with recurrent flare-ups.
Simplified Flow of Psoriasis Pathophysiology
Clinical Features Resulting from the Pathophysiology
The underlying immune-mediated inflammation and accelerated epidermal turnover produce the characteristic manifestations of psoriasis, including:
- Well-defined erythematous plaques covered with silvery-white scales
- Dry, cracked skin that may bleed
- Pruritus (itching) or burning sensation
- Thickened epidermis (acanthosis)
- Nail pitting, onycholysis, and discoloration
- Joint pain and swelling in patients with psoriatic arthritis
- Recurrent episodes of remission and relapse
Conclusion
Psoriasis is a chronic, immune-mediated inflammatory disease in which genetic susceptibility and environmental triggers initiate an abnormal immune response. The IL-23/Th17/IL-17 axis, along with TNF-α, plays the central role in driving the disease. Activation of these inflammatory pathways causes rapid keratinocyte proliferation, abnormal epidermal differentiation, angiogenesis, and chronic inflammation, resulting in the formation of characteristic erythematous, scaly plaques. Understanding this pathophysiology has transformed psoriasis treatment, leading to the development of highly targeted biologic therapies that inhibit TNF-α, IL-17, and IL-23, providing effective long-term disease control for many patients.