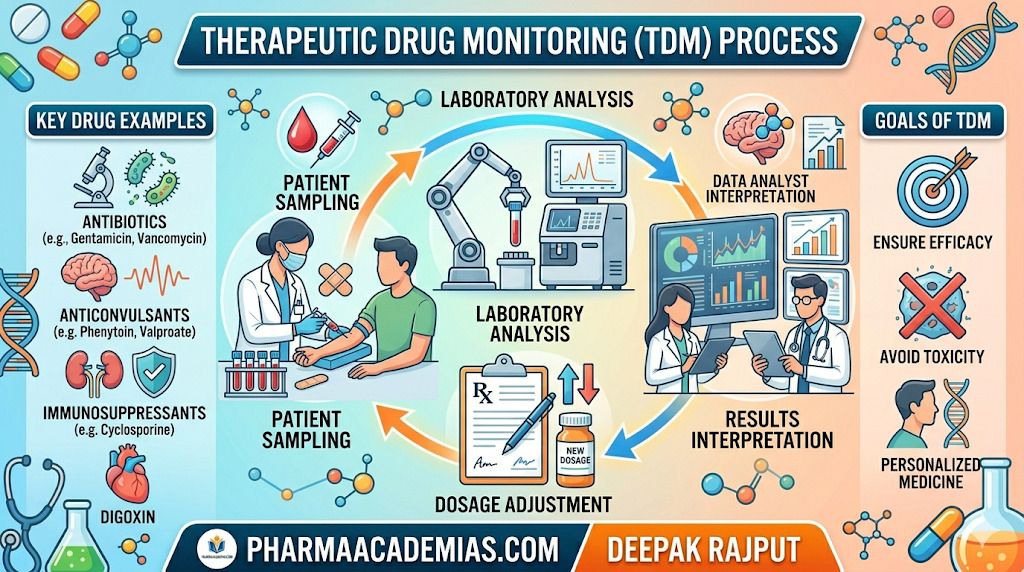
Therapeutic Drug Monitoring (TDM) is the clinical practice of measuring the concentration of selected drugs in blood, plasma, or other biological fluids at specific intervals to maintain the drug level within the therapeutic range, that is, the concentration at which the medicine produces maximum benefit with minimum toxicity. It is a major tool of individualized or precision pharmacotherapy, especially for medicines that have a narrow therapeutic index, marked pharmacokinetic variability, nonlinear kinetics, or serious dose-related adverse effects. TDM is especially important for drugs such as aminoglycosides, vancomycin, digoxin, lithium, phenytoin, valproate, carbamazepine, cyclosporine, tacrolimus, methotrexate, and certain antifungals.
Unlike routine dose adjustment based only on symptoms, TDM links the measured blood concentration of the drug with the patient’s clinical response, allowing the clinician to optimize therapy scientifically. This is why TDM is considered one of the strongest pillars of clinical pharmacy, pharmacokinetics, and rational drug therapy.
Need for Therapeutic Drug Monitoring
The need for therapeutic drug monitoring arises because the same dose of a medicine may produce very different blood levels in different patients. These differences occur due to age, body weight, organ function, genetics, disease state, and drug interactions.
The most important need is in drugs with a narrow therapeutic window, where a small difference in concentration can change the outcome from effective treatment to toxicity. For example, a slight increase in digoxin or lithium concentration may produce serious toxic effects, while a slight decrease may lead to therapeutic failure.
TDM is also needed when there is large interpatient pharmacokinetic variability. Some patients metabolize medicines rapidly, while others eliminate them slowly. In such situations, standard doses cannot be safely applied to all patients.
Another major need is seen in drugs with poorly defined clinical endpoints. For instance, in anticonvulsant therapy, it may take days or weeks to know whether seizure control is adequate. Measuring plasma levels gives a faster and more reliable basis for dose adjustment.
TDM is highly useful in the prevention of drug toxicity, especially in nephrotoxic and ototoxic medicines like aminoglycosides and vancomycin. It helps ensure that peak levels are sufficient for efficacy and trough levels are low enough to prevent toxicity.
It is also required in cases of:
- suspected non-compliance
- therapeutic failure
- overdose or poisoning
- organ dysfunction
- drug-drug interactions
- critically ill patients
- pediatric and geriatric patients
- transplant recipients
- ICU patients with fluctuating renal function
In modern therapeutics, the need for TDM has expanded beyond toxicity prevention to include dose individualization, antimicrobial stewardship, resistance prevention, and precision medicine.
Factors to Be Considered During Therapeutic Drug Monitoring
The success of TDM depends not merely on measuring the drug concentration, but on correct interpretation in the context of the patient and the sampling conditions.
The first and most critical factor is the correct timing of sample collection. Blood must be collected at the appropriate time, such as peak level, trough level, or steady-state concentration, depending on the drug. If the sample is taken too early or too late, the result may be misleading.
The dose regimen must always be reviewed carefully, including dose, frequency, route, infusion time, and duration of therapy. Without knowing the exact dosage schedule, the measured level cannot be interpreted properly.
The patient’s clinical status is equally important. The measured concentration must always be correlated with:
- therapeutic response
- signs of toxicity
- disease severity
- organ function
- hydration status
- vital signs
A laboratory value alone should never be used in isolation.
Another key factor is pharmacokinetic variability, including absorption, distribution, metabolism, and excretion. Renal and hepatic impairment can drastically alter drug clearance and therefore must be considered before changing doses.
The patient-specific variables that influence TDM include age, body weight, pregnancy, plasma protein levels, burns, obesity, critical illness, and genetic polymorphism. For example, hypoalbuminemia can alter free phenytoin levels even when total drug concentration appears normal.
Drug interactions are another major consideration. Medicines that induce or inhibit liver enzymes can significantly increase or decrease plasma concentrations of monitored drugs.
The analytical method and laboratory reliability are also essential. TDM requires validated, accurate, and sensitive methods such as:
- immunoassay
- HPLC
- LC-MS/MS
- gas chromatography
Poor sample handling, wrong anticoagulant use, hemolysis, or storage errors may produce false results.
Thus, proper TDM requires integration of clinical pharmacology, laboratory science, patient assessment, and therapeutic judgment.
Indian Scenario for Therapeutic Drug Monitoring
The Indian scenario of therapeutic drug monitoring is highly important from an academic and practical pharmacy perspective.
In India, TDM has gradually evolved from a limited laboratory service to an important part of clinical pharmacology, hospital pharmacy, and personalized medicine, but its use is still underutilized compared with developed healthcare systems.
Historically, TDM services in India began in major tertiary care institutions such as King Edward Memorial Hospital, Mumbai, followed by centers like Christian Medical College, Vellore, and PGIMER Chandigarh. Today, advanced TDM services are available in selected AIIMS institutions, transplant centers, oncology hospitals, neurology centers, and large corporate hospitals.
The Indian need for TDM is particularly high because of:
- wide patient diversity
- nutritional deficiencies
- high burden of infectious diseases
- tuberculosis therapy
- transplant medicine
- epilepsy management
- antifungal therapy
- ICU antimicrobial use
- variable pharmacogenomics
- frequent polypharmacy
TDM is especially relevant in India for:
- antiepileptic drugs
- tacrolimus and cyclosporine
- aminoglycosides
- vancomycin
- anti-TB medicines
- methotrexate
- anticancer drugs
Despite its importance, India faces several challenges:
- limited infrastructure in district and rural hospitals
- high assay cost
- lack of trained clinical pharmacologists
- shortage of clinical pharmacists
- absence of uniform national guidelines
- delayed reporting time
- inadequate awareness among prescribers
- limited access outside teaching hospitals
These barriers reduce the widespread implementation of TDM in routine practice.
However, the Indian future is promising. Recent reviews strongly recommend:
- national TDM centers
- regional reference laboratories
- pharmacokinetic consultation services
- integration with hospital information systems
- AI-assisted dose optimization
- pharmacist-led TDM services
- antimicrobial stewardship linked TDM
This is expected to make TDM a core component of precision medicine in India over the coming years.
Conclusion
Therapeutic Drug Monitoring is a scientifically guided method of optimizing drug therapy by measuring plasma drug concentrations and correlating them with patient response.
Its need is greatest in drugs with narrow therapeutic index, variable pharmacokinetics, organ dysfunction, and toxicity risk. Successful TDM depends on careful consideration of sampling time, dose regimen, patient variables, organ function, laboratory accuracy, and clinical interpretation.
In the Indian healthcare scenario, TDM is expanding rapidly in tertiary hospitals, transplant units, oncology, neurology, and infectious disease care, though infrastructure and standardization challenges still remain.
Overall, TDM plays a vital role in safe, effective, and individualized pharmacotherapy, making it one of the most valuable tools in modern hospital and clinical pharmacy practice.