Morphology of Cell Injury: The morphology of cell injury refers to the structural and functional changes that occur in cells when they are exposed to physiological stress or harmful stimuli. Cells are constantly subjected to changes in their internal and external environment. Under normal conditions, they adapt to these changes to maintain their normal function and ensure survival. However, when the stress exceeds the adaptive capacity of the cell or the injurious stimulus is severe or prolonged, cellular injury develops. Initially, these changes may be reversible, but persistent injury eventually leads to irreversible damage and cell death. Pharmaacademias.com
Morphological changes in injured cells can be observed using light and electron microscopy and often provide important clues regarding the nature and severity of disease. Before a cell dies, it usually undergoes a series of adaptive changes that help it survive under unfavorable conditions. If adaptation fails, the cell progresses through reversible injury, irreversible injury, and finally cell death.
Adaptive Changes of Cells
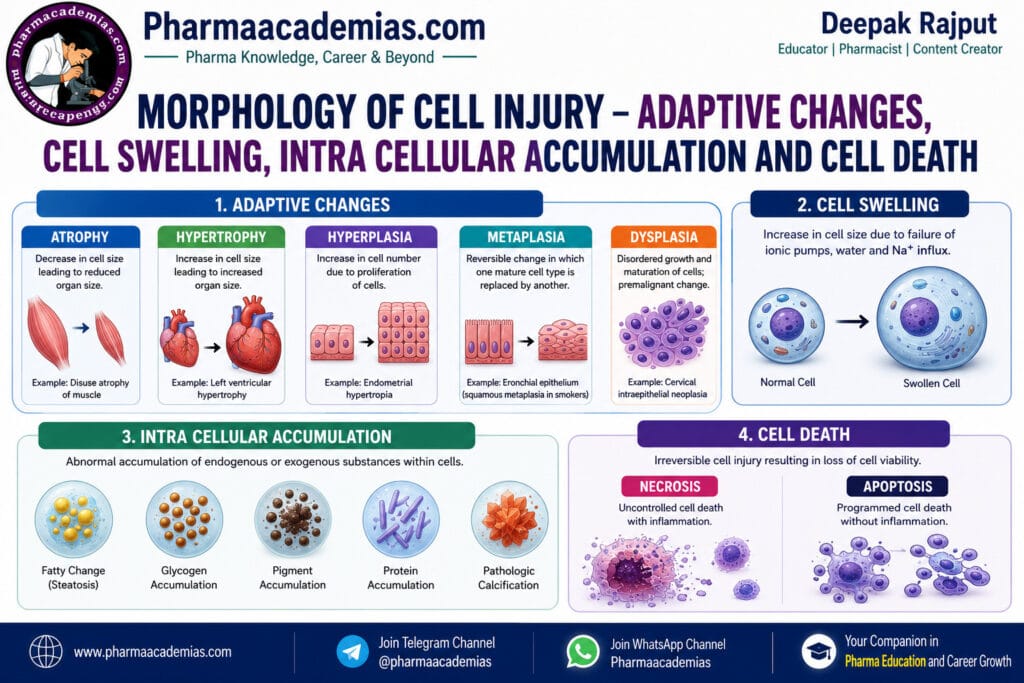
Cellular adaptation is the process by which cells adjust their structure, function, or number in response to physiological demands or pathological stress. These adaptations enable cells to survive in altered environments while maintaining their essential functions. The major adaptive changes include atrophy, hypertrophy, hyperplasia, metaplasia, and dysplasia.
1. Atrophy
Atrophy is the decrease in the size of a cell, tissue, or organ due to a reduction in the size and number of cellular components. As a result, the affected organ becomes smaller and its functional capacity is reduced. Atrophy is generally an adaptive response that allows the cell to survive under conditions of reduced workload or limited nutrient supply.
Atrophy may occur under both physiological and pathological conditions. Physiological atrophy is a normal part of development and ageing, such as the shrinkage of the thymus after puberty or the involution of the uterus after childbirth. Pathological atrophy occurs as a result of disuse, denervation, diminished blood supply, inadequate nutrition, loss of endocrine stimulation, pressure, or ageing.
The mechanisms responsible for atrophy include decreased protein synthesis, increased protein degradation through the ubiquitin-proteasome pathway, and activation of autophagy, in which damaged cellular organelles are digested within lysosomes to provide nutrients for cell survival.
Common examples include skeletal muscle atrophy after prolonged immobilization, cerebral atrophy in Alzheimer’s disease, renal atrophy due to chronic ischemia, and testicular atrophy following hormonal deficiency.
Although atrophy is generally reversible if the underlying cause is corrected early, prolonged atrophy may become irreversible because of permanent loss of cells and tissue function.
2. Hypertrophy
Hypertrophy is an increase in the size of individual cells, resulting in enlargement of the affected organ or tissue without an increase in the number of cells. This adaptation occurs when cells are unable to divide or when increased functional demand requires greater cellular activity.
Hypertrophy develops through increased synthesis of structural proteins and intracellular organelles, leading to enlargement of the cytoplasm and increased functional capacity of the cell. The process is regulated by mechanical stress, growth factors, and hormones.
Physiological hypertrophy occurs during normal body development or increased physical activity. For example, enlargement of skeletal muscles in athletes occurs due to regular exercise, while enlargement of the uterus during pregnancy results from hormonal stimulation.
Pathological hypertrophy commonly occurs in the heart. In patients with hypertension or valvular heart disease, cardiac muscle cells enlarge because they must generate greater force to pump blood against increased resistance. Initially, this adaptation improves cardiac function; however, prolonged hypertrophy eventually leads to heart failure due to increased oxygen demand and reduced efficiency.
Hypertrophy is therefore considered a beneficial adaptive response in its early stages but may become harmful if excessive or prolonged.
3. Hyperplasia
Hyperplasia is an increase in the number of cells within a tissue or organ due to increased cellular proliferation. Unlike hypertrophy, where individual cells become larger, hyperplasia results from cell division, leading to enlargement of the affected tissue.
Hyperplasia occurs only in tissues whose cells retain the ability to divide. It is regulated by growth factors, hormones, and cytokines that stimulate DNA synthesis and cell proliferation.
Physiological hyperplasia occurs as a normal response to hormonal stimulation or increased functional demand. During pregnancy, the glandular tissue of the breast undergoes hyperplasia to prepare for milk production. Similarly, regeneration of the liver following partial surgical removal occurs through compensatory hyperplasia.
Pathological hyperplasia develops because of excessive hormonal stimulation or abnormal growth factor activity. Examples include endometrial hyperplasia caused by excessive estrogen stimulation and benign prostatic hyperplasia (BPH), in which the prostate gland enlarges due to hormonal influences in elderly men.
Hyperplasia is usually reversible after removal of the stimulating factor. However, persistent pathological hyperplasia may increase the risk of developing certain cancers, particularly in tissues such as the endometrium.
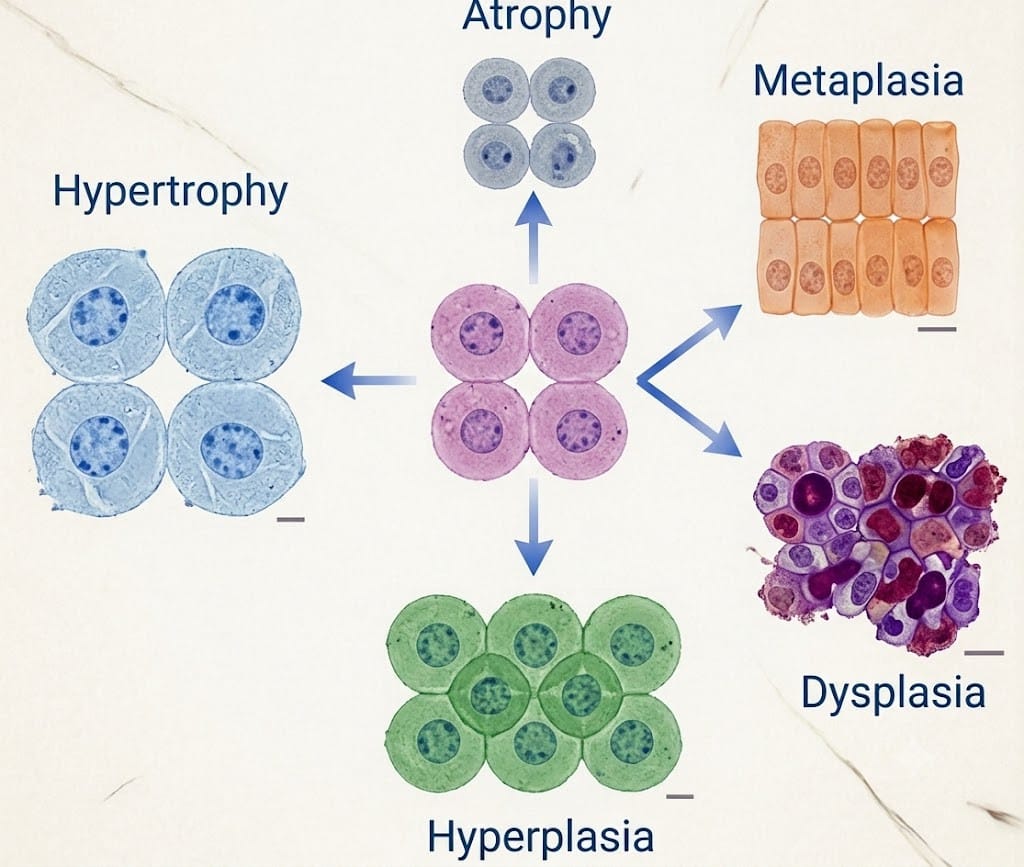
4. Metaplasia
Metaplasia is a reversible adaptive process in which one mature differentiated cell type is replaced by another mature cell type better able to withstand adverse environmental conditions. This transformation occurs through the reprogramming of stem cells rather than direct conversion of one mature cell into another.
Metaplasia develops as a protective mechanism against chronic irritation or inflammation. Although the new cell type is more resistant to injury, it often loses the specialized functions of the original cells, thereby reducing normal tissue function.
One of the most common examples is squamous metaplasia in the respiratory tract of chronic smokers. Normally, the bronchi are lined by ciliated columnar epithelial cells that remove mucus and inhaled particles. Continuous exposure to cigarette smoke causes these cells to be replaced by stratified squamous epithelium, which is more resistant to irritation but lacks cilia, reducing the efficiency of mucociliary clearance.
Another example is Barrett’s esophagus, in which the normal stratified squamous epithelium of the lower esophagus is replaced by columnar epithelium because of chronic gastroesophageal reflux disease (GERD).
Metaplasia is generally reversible if the injurious stimulus is removed. However, persistent metaplasia may progress to dysplasia and eventually carcinoma.
5. Dysplasia
Dysplasia refers to abnormal growth, maturation, and organization of cells within a tissue. It is characterized by variations in cell size and shape, enlarged hyperchromatic nuclei, increased mitotic activity, and loss of normal cellular architecture.
Unlike metaplasia, dysplasia is not considered a true adaptive response but rather a premalignant change that may precede the development of cancer. Dysplasia most commonly occurs in epithelial tissues exposed to chronic irritation or persistent inflammation.
Examples include cervical dysplasia associated with persistent human papillomavirus (HPV) infection, bronchial dysplasia in chronic smokers, and dysplastic changes in the oral mucosa of tobacco users.
Mild dysplasia may regress if the underlying cause is eliminated. However, severe dysplasia has a high risk of progressing to carcinoma if left untreated. Therefore, early detection through screening programs such as the Pap smear is essential.
Cell Swelling
Cell swelling, also known as hydropic change or cloudy swelling, is the earliest and most common morphological manifestation of reversible cell injury. It occurs when the cell loses its ability to regulate the movement of sodium and water across the plasma membrane.
Normally, the sodium-potassium ATPase pump maintains ionic balance by actively transporting sodium out of the cell and potassium into the cell. During hypoxia, ischemia, or ATP depletion, this pump fails, causing sodium and water to accumulate within the cytoplasm. As a result, the cell enlarges, and intracellular organelles such as the endoplasmic reticulum and mitochondria become swollen.
Microscopically, swollen cells appear enlarged with pale, vacuolated cytoplasm. Electron microscopy reveals distended endoplasmic reticulum, mitochondrial swelling, and membrane blebbing.
Cell swelling is generally reversible if oxygen supply and ATP production are restored. However, persistent swelling eventually progresses to irreversible cellular injury and cell death.
Intracellular Accumulation
Intracellular accumulation refers to the abnormal build-up of substances within the cytoplasm, nucleus, or lysosomes of cells. These substances may be produced normally but accumulate because of defective metabolism, impaired transport, excessive production, or inability of the cell to degrade them.
The most common intracellular accumulations include lipids (fat), proteins, glycogen, pigments, and minerals.
Fat accumulation, also known as fatty change (steatosis), occurs mainly in the liver and heart. It is commonly associated with alcohol abuse, obesity, diabetes mellitus, malnutrition, and hypoxia. Excess triglycerides accumulate within hepatocytes, causing enlargement of the liver and impaired liver function.
Protein accumulation may occur in kidney diseases, plasma cell disorders, and chronic inflammation. Glycogen accumulation is observed in uncontrolled diabetes mellitus and inherited glycogen storage diseases.
Pigments may be either endogenous or exogenous. Endogenous pigments include melanin, lipofuscin, and hemosiderin, whereas exogenous pigments include carbon particles deposited in the lungs of smokers or individuals exposed to air pollution.
Excessive intracellular accumulation interferes with normal cellular metabolism and may eventually lead to cellular dysfunction and injury.
Cell Death
When cellular injury becomes severe and irreversible, the cell undergoes cell death. Cell death is the final outcome of irreversible cellular injury and occurs primarily through necrosis or apoptosis.
Necrosis
Necrosis is an uncontrolled form of cell death resulting from severe injury such as ischemia, infections, toxins, trauma, or chemical exposure. During necrosis, the plasma membrane ruptures, intracellular enzymes leak into the surrounding tissues, and an inflammatory response develops.
Morphologically, necrotic cells exhibit increased cytoplasmic eosinophilia, disruption of cellular architecture, and characteristic nuclear changes such as pyknosis (nuclear shrinkage), karyorrhexis (fragmentation of the nucleus), and karyolysis (dissolution of the nucleus).
Common examples include myocardial infarction, gangrene, burns, and cerebral infarction.
Apoptosis
Apoptosis is a programmed and highly regulated form of cell death that removes unwanted, damaged, or aged cells without causing inflammation. It plays an essential role in embryonic development, maintenance of tissue homeostasis, immune regulation, and elimination of genetically damaged cells.
During apoptosis, the cell shrinks, chromatin condenses, DNA fragments, and membrane-bound apoptotic bodies are formed. These apoptotic bodies are rapidly engulfed by macrophages without releasing intracellular contents, thereby preventing inflammation.
Apoptosis occurs during normal physiological processes such as embryogenesis and tissue remodeling, as well as in pathological conditions including DNA damage, viral infections, and certain neurodegenerative diseases.
Clinical Significance
The study of the morphology of cell injury is essential for understanding the development and progression of many diseases. Adaptive changes such as atrophy, hypertrophy, hyperplasia, and metaplasia initially help cells survive adverse conditions, but persistent stress may lead to dysplasia, irreversible injury, and cancer. Similarly, cell swelling and intracellular accumulation are important indicators of reversible injury, whereas necrosis and apoptosis represent the final outcomes of severe cellular damage. Recognition of these morphological changes assists clinicians and pathologists in diagnosing diseases, assessing disease severity, and planning appropriate treatment strategies.
Conclusion
The morphology of cell injury encompasses a series of structural and functional changes that occur when cells respond to stress or harmful stimuli. Cells initially adapt through atrophy, hypertrophy, hyperplasia, metaplasia, and dysplasia to maintain survival. If the injurious stimulus persists, cell swelling and intracellular accumulation develop as manifestations of reversible injury. Continued or severe injury ultimately results in cell death, either by necrosis, which is associated with inflammation, or apoptosis, a regulated process that eliminates damaged cells without causing inflammation. Understanding these morphological changes is fundamental to the study of human anatomy, physiology, and pathophysiology, as they form the basis for the development and progression of numerous diseases.
Editorial Note
This article has been carefully researched and written by Deepak Rajput with a focus on accuracy, clarity, and evidence-based healthcare information.