Skyrizi : Autoimmune diseases have long challenged both patients and healthcare professionals due to their chronic nature, unpredictable flare-ups, and significant impact on quality of life. Conditions such as plaque psoriasis, psoriatic arthritis, Crohn’s disease, and ulcerative colitis result from an overactive immune system attacking the body’s own tissues. While conventional therapies often reduce symptoms temporarily, many patients continue to experience relapses, incomplete disease control, or adverse effects.
The introduction of biologic therapies has transformed autoimmune disease management by targeting specific immune pathways instead of broadly suppressing the immune system. Among the newest and most effective biologics is Skyrizi® (Risankizumab-rzaa), a monoclonal antibody specifically designed to inhibit Interleukin-23 (IL-23)—a key inflammatory cytokine involved in autoimmune diseases.
Since receiving its first FDA approval in 2019, Skyrizi has rapidly become one of the most successful IL-23 inhibitors because of its impressive clinical efficacy, convenient dosing schedule, and favorable safety profile. Clinical trials have demonstrated that a large proportion of patients achieve almost complete or complete skin clearance while maintaining long-term disease control with only four maintenance doses per year after the initial loading phase.
This article provides a comprehensive overview of Skyrizi, including its mechanism of action, approved indications, pharmacology, clinical evidence, dosing regimen, safety profile, and future role in autoimmune disease treatment.
What is Skyrizi?
Skyrizi is the brand name of risankizumab-rzaa, a humanized IgG1 monoclonal antibody developed to selectively inhibit the p19 subunit of IL-23. Unlike older biologics that block multiple cytokines, risankizumab specifically targets IL-23 without directly inhibiting IL-12, allowing for more selective immune modulation.
The medicine is administered as a subcutaneous injection and is approved for adults with autoimmune inflammatory diseases. According to the prescribing information in your uploaded document, Skyrizi was initially approved for:
- Moderate-to-severe plaque psoriasis
- Active psoriatic arthritis
The prescribing information also details its recommended dosing schedule, contraindications, safety precautions, and efficacy data.
Understanding Autoimmune Inflammation
The human immune system protects the body against harmful microorganisms such as bacteria, viruses, and fungi. However, in autoimmune diseases, immune cells mistakenly attack healthy tissues, leading to persistent inflammation.
In psoriasis, immune cells become overactive and stimulate excessive skin cell proliferation. Normally, skin cells mature over approximately one month, but in psoriasis this process may occur within only a few days, resulting in:
- Thick scaly plaques
- Persistent redness
- Itching
- Pain
- Skin cracking
- Bleeding
Similarly, in psoriatic arthritis, chronic inflammation damages joints, tendons, and surrounding tissues, causing pain, swelling, stiffness, and progressive disability.
Scientific research has identified the IL-23/Th17 pathway as one of the central drivers of these inflammatory processes.
The IL-23 Pathway: Why It Matters
Interleukin-23 (IL-23) is a cytokine produced primarily by activated dendritic cells and macrophages. It plays a crucial role in maintaining and expanding Th17 lymphocytes, a subset of T-helper cells responsible for producing several pro-inflammatory cytokines.
These cytokines include:
- IL-17A
- IL-17F
- IL-22
- TNF-α
- GM-CSF
Together, they promote chronic inflammation, excessive keratinocyte proliferation, recruitment of immune cells into skin and joints, and ongoing tissue damage.
Blocking IL-23 interrupts this inflammatory cascade near its source, reducing downstream cytokine production and helping restore immune balance.
Mechanism of Action of Skyrizi
Skyrizi works by selectively binding to the p19 subunit of IL-23, preventing IL-23 from interacting with its receptor on immune cells. This inhibition suppresses activation and survival of pathogenic Th17 cells, leading to reduced production of inflammatory cytokines and decreased tissue inflammation.
Unlike medications that broadly suppress immune function, this targeted approach focuses on a specific inflammatory pathway involved in autoimmune disease.
The result is:
- Reduced skin inflammation
- Decreased plaque formation
- Improvement in joint inflammation
- Lower immune-mediated tissue damage
- Long-lasting disease control
FDA-Approved Indications
According to the prescribing information, Skyrizi is approved for adults with:
1. Moderate-to-Severe Plaque Psoriasis: Patients eligible for systemic therapy or phototherapy may receive Skyrizi as a biologic treatment. The medication significantly improves skin clearance and reduces disease severity.
2. Active Psoriatic Arthritis: Skyrizi can be administered either as monotherapy or in combination with non-biologic disease-modifying antirheumatic drugs (DMARDs). Clinical studies have shown meaningful improvements in joint symptoms, physical function, and quality of life.
Why IL-23 Inhibition Is Considered a Major Advancement
Earlier biologic therapies targeted broader immune mediators such as TNF-α or both IL-12 and IL-23. While effective, these approaches may influence wider immune functions.
Selective IL-23 inhibition offers several theoretical and clinical advantages:
- Highly targeted immune modulation
- Durable clinical responses
- Less frequent maintenance dosing
- Sustained skin clearance
- Improved patient adherence
- Favorable long-term safety profile observed in clinical trials
These characteristics have positioned Skyrizi as one of the leading biologic options for immune-mediated inflammatory diseases.
Clinical Effectiveness in Plaque Psoriasis
The pivotal Phase 3 clinical trials enrolled adults with moderate-to-severe plaque psoriasis characterized by:
- Body Surface Area (BSA) involvement ≥10%
- PASI score ≥12
- Static Physician Global Assessment (sPGA) ≥3
Patients treated with Skyrizi achieved remarkable improvements compared with placebo.
At Week 16:
- Up to 88% achieved clear or almost clear skin (sPGA 0/1).
- Approximately 75% achieved PASI 90.
- Up to 51% achieved complete skin clearance (PASI 100).
Importantly, these responses were maintained through Week 52 in the majority of patients who continued therapy.
These findings established Skyrizi as one of the most effective biologics available for plaque psoriasis treatment.
Clinical Evidence Supporting Skyrizi
One of the primary reasons Skyrizi has become a preferred biologic for immune-mediated inflammatory diseases is the strength of its clinical evidence. Multiple large, randomized, double-blind, placebo-controlled Phase III clinical trials have consistently demonstrated high efficacy, durable responses, and an acceptable safety profile.
The pivotal psoriasis trials—PsO-1, PsO-2, PsO-3, and PsO-4—included more than 2,100 adults with moderate-to-severe plaque psoriasis. Eligible participants had at least 10% body surface area involvement, a Psoriasis Area and Severity Index (PASI) score of 12 or greater, and moderate-to-severe disease as measured by the static Physician’s Global Assessment (sPGA).
Results in Plaque Psoriasis
The efficacy of Skyrizi became evident as early as Week 16.
Clear or Almost Clear Skin (sPGA 0/1)
Approximately 84–88% of patients receiving Skyrizi achieved clear or almost clear skin compared with only 5–8% receiving placebo.
PASI 90 Response
Nearly three out of every four treated patients achieved at least a 90% improvement in disease severity.
- Skyrizi: approximately 75%
- Placebo: 2–5%
These differences were statistically significant and clinically meaningful.
Complete Skin Clearance (PASI 100)
Perhaps the most impressive finding was complete clearance of psoriatic lesions.
Up to half of all patients achieved PASI 100 by Week 16, demonstrating complete disappearance of visible plaques.
Long-Term Disease Control
Unlike many therapies that lose effectiveness over time, Skyrizi demonstrated remarkable durability.
Among patients who achieved PASI 100 at Week 16:
- Around 80% maintained complete skin clearance through Week 52.
Among PASI 90 responders:
- Approximately 88% maintained their response after one year of treatment.
These findings suggest that selective IL-23 inhibition provides sustained suppression of chronic inflammation.
Clinical Studies in Psoriatic Arthritis
Skyrizi has also shown significant efficacy in active psoriatic arthritis (PsA).
Two major Phase III studies (PsA-1 and PsA-2) enrolled more than 1,400 adults with active disease. Participants had:
- Active joint inflammation
- Swollen and tender joints
- Long-standing disease
- Many had concomitant plaque psoriasis
Patients received 150 mg of Skyrizi at Weeks 0, 4, and 16, followed by maintenance therapy every 12 weeks.
Improvement in Joint Symptoms
The primary endpoint was achievement of the American College of Rheumatology 20 (ACR20) response.
At Week 24:
PsA-1 Trial
- Placebo: 33.5%
- Skyrizi: 57.3%
PsA-2 Trial
- Placebo: 26.5%
- Skyrizi: 51.3%
These results confirmed significantly better control of joint inflammation with Skyrizi than placebo.
Improvement Beyond Joint Counts
Clinical improvements extended well beyond swollen and tender joints.
Patients experienced improvements in:
- Physical function
- Daily activities
- Pain
- Fatigue
- Enthesitis
- Dactylitis
- Quality of life
- Skin lesions
The Health Assessment Questionnaire Disability Index (HAQ-DI) also improved significantly compared with placebo.
Pharmacokinetics: Understanding the pharmacokinetic profile helps explain the convenient dosing schedule of Skyrizi.
Bioavailability: Following subcutaneous administration, the absolute bioavailability is approximately 89%.
Time to Peak Concentration: Maximum plasma concentration is generally reached within:
3–14 days after injection.
Distribution: The steady-state volume of distribution is approximately:
11.2 L
indicating limited distribution outside the vascular and extracellular compartments.
Elimination Half-Life: One of Skyrizi’s greatest advantages is its long elimination half-life of approximately:
28 days
This prolonged half-life supports maintenance dosing every 12 weeks after the loading doses.
Dosage and Administration
According to the prescribing information, the recommended dosage for both plaque psoriasis and psoriatic arthritis is:
- Week 0 – 150 mg
- Week 4 – 150 mg
- Every 12 weeks thereafter – 150 mg
Administration is performed by subcutaneous injection.
Patients may self-administer the medication after receiving appropriate training from healthcare professionals.
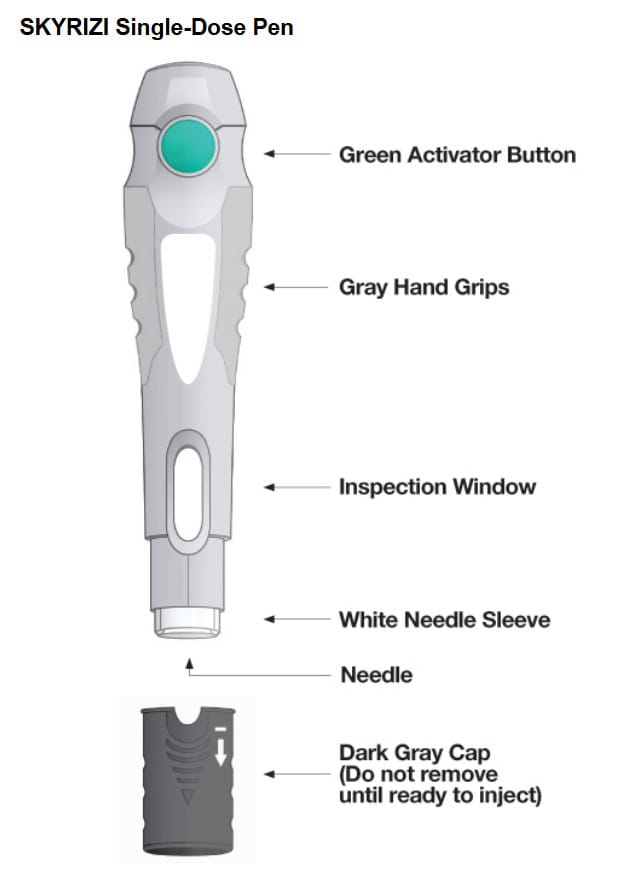
Available Formulations
Skyrizi is available as:
- 150 mg/mL prefilled pen
- 150 mg/mL prefilled syringe
- 75 mg/0.83 mL prefilled syringe
For the 75 mg presentation, two injections are required to deliver the full 150 mg dose.
Mechanistic Advantages Over Older Biologics
Compared with first-generation biologics, Skyrizi offers several advantages:
| Feature | Skyrizi |
| Target | IL-23 p19 |
| Administration | Subcutaneous |
| Maintenance Frequency | Every 12 weeks |
| Immune Targeting | Highly selective |
| Complete Skin Clearance | High PASI100 rates |
| Long Half-life | ~28 days |
Selective inhibition of IL-23 reduces downstream inflammatory cytokines while preserving other immune pathways, contributing to durable efficacy and an acceptable safety profile.
Safety Profile of Skyrizi
Like all biologic therapies, Skyrizi is generally well tolerated but is associated with certain adverse effects and precautions that healthcare providers and patients should understand before initiating treatment. Overall, long-term clinical trials have shown a favorable benefit-risk profile, with most adverse events being mild to moderate in severity.
Common Side Effects
The most frequently reported adverse reactions (occurring in at least 1% of patients) include:
- Upper respiratory tract infections
- Headache
- Fatigue
- Injection-site reactions
- Fungal skin infections (tinea)
In pooled clinical trials involving more than 1,300 patients treated with Skyrizi, upper respiratory infections were the most commonly observed adverse event, occurring in approximately 13% of treated patients.
Injection-Site Reactions
Some patients may experience temporary reactions such as:
- Redness
- Mild swelling
- Pain
- Bruising
- Itching
- Warmth
These reactions are generally self-limiting and resolve without specific treatment.
Serious Adverse Effects
Although uncommon, serious adverse events can occur.
Serious Infections
Because Skyrizi modifies immune function, patients have an increased susceptibility to infections.
Serious infections reported during clinical trials included:
- Cellulitis
- Osteomyelitis
- Sepsis
- Herpes zoster
- Pneumonia
Patients with active infections should not begin therapy until the infection has completely resolved.
Hypersensitivity Reactions
Rare but serious allergic reactions have been reported, including:
- Anaphylaxis
- Facial swelling
- Generalized rash
- Urticaria
- Difficulty breathing
Treatment should be discontinued immediately if severe hypersensitivity develops.
Tuberculosis Screening
Before initiating Skyrizi, every patient should undergo evaluation for tuberculosis (TB).
Patients with:
- Active tuberculosis
- Untreated latent tuberculosis
- Previous inadequately treated TB
require appropriate medical assessment before therapy begins.
During treatment, patients should continue to be monitored for signs and symptoms of tuberculosis.
Vaccination Recommendations
Live vaccines should not be administered during treatment with Skyrizi because immune modulation may increase the risk of vaccine-related infection.
Recommended vaccinations should ideally be completed before starting therapy.
Contraindications
According to the prescribing information, Skyrizi is contraindicated in individuals with:
- A history of serious hypersensitivity to risankizumab-rzaa
- Allergy to any formulation component
No other absolute contraindications are listed in the FDA-approved labeling.
Pregnancy and Breastfeeding
Human data regarding the use of Skyrizi during pregnancy remain limited.
Animal studies did not demonstrate maternal toxicity, although increased fetal or infant loss was observed at high exposure levels in cynomolgus monkeys. The clinical significance of these findings in humans is uncertain. A pregnancy exposure registry is available to monitor outcomes in women exposed to Skyrizi during pregnancy.
There are currently no adequate human data regarding secretion into breast milk or its effects on nursing infants. Healthcare providers should weigh the benefits of treatment against potential risks when prescribing during lactation.
Drug Interactions
Unlike many conventional immunosuppressive drugs, Skyrizi has demonstrated a relatively low potential for clinically significant drug interactions.
Clinical pharmacology studies found no meaningful changes in the exposure of common CYP450 substrates such as:
- Warfarin
- Omeprazole
- Midazolam
- Metoprolol
- Caffeine
However, concomitant use of live vaccines should be avoided.
Comparing Skyrizi with Other Biologics
| Feature | Skyrizi | Humira | Cosentyx | Stelara | Tremfya |
| Target | IL-23 p19 | TNF-α | IL-17A | IL-12/23 | IL-23 p19 |
| Maintenance Dosing | Every 12 weeks | Every 2 weeks | Every 4 weeks | Every 12 weeks | Every 8 weeks |
| Administration | SC | SC | SC | SC/IV | SC |
| Complete Skin Clearance | Very High | Moderate | High | High | Very High |
| Selectivity | Very High | Broad | Moderate | Moderate | Very High |
Because of its selective IL-23 inhibition and infrequent maintenance dosing, Skyrizi is considered one of the most convenient biologic therapies for eligible patients.
Emerging Uses of Skyrizi
Research over the past few years has expanded the clinical applications of risankizumab beyond psoriasis and psoriatic arthritis. It is now also approved in several regions for inflammatory bowel diseases such as Crohn’s disease and ulcerative colitis, reflecting the important role of IL-23 in intestinal inflammation. Ongoing studies are evaluating its long-term efficacy, safety, and potential use in additional immune-mediated disorders.
Frequently Asked Questions (FAQs)
How does Skyrizi work?
Skyrizi blocks the IL-23 p19 subunit, reducing inflammatory signaling involved in autoimmune diseases.
How often is Skyrizi administered?
After the initial doses at Weeks 0 and 4, maintenance injections are given every 12 weeks.
Can patients inject Skyrizi at home?
Yes. Following appropriate training from a healthcare professional, patients may self-administer Skyrizi using a prefilled pen or syringe.
What are the most common side effects?
Upper respiratory infections, headache, fatigue, injection-site reactions, and fungal skin infections are the most frequently reported adverse events.
Should tuberculosis screening be performed before treatment?
Yes. All patients should be evaluated for tuberculosis before starting Skyrizi therapy.
Conclusion
Skyrizi (risankizumab-rzaa) represents a significant advancement in the treatment of immune-mediated inflammatory diseases. By selectively inhibiting the IL-23 p19 pathway, it provides highly targeted immune modulation while maintaining durable clinical responses and a convenient dosing schedule.
Clinical trials have demonstrated high rates of skin clearance in plaque psoriasis, meaningful improvements in joint symptoms for psoriatic arthritis, and sustained efficacy with maintenance dosing every 12 weeks. Its favorable safety profile, low incidence of serious adverse events, and limited drug-drug interactions have established Skyrizi as one of the leading biologic therapies in modern dermatology and rheumatology.
As research continues to expand its indications into inflammatory bowel disease and potentially other immune-mediated disorders, Skyrizi is expected to play an increasingly important role in precision medicine and targeted immunotherapy.
References
- U.S. Food and Drug Administration. SKYRIZI (risankizumab-rzaa) Prescribing Information. Revised 2022. (Primary reference: uploaded FDA label.)
- Gordon KB, et al. Lancet. Phase III trials of risankizumab in plaque psoriasis.
- Reich K, et al. New England Journal of Medicine. Risankizumab versus ustekinumab.
- Warren RB, et al. Long-term efficacy of risankizumab in psoriasis.
- Mease PJ, et al. Risankizumab for active psoriatic arthritis.
- Blauvelt A, et al. IL-23 inhibition in chronic inflammatory diseases.
- ClinicalTrials.gov: PsO-1 (NCT02684370).
- ClinicalTrials.gov: PsO-2 (NCT02684357).
- ClinicalTrials.gov: PsO-3 (NCT02672852).
- ClinicalTrials.gov: PsA-1 (NCT03675308).
- ClinicalTrials.gov: PsA-2 (NCT03671148).