
Diabetes Mellitus is a chronic metabolic disorder characterized by persistent hyperglycemia due to defects in insulin secretion, insulin action, or both. It is one of the most significant non-communicable diseases worldwide and represents a major public health burden due to its increasing prevalence, long-term complications, and association with cardiovascular mortality. The disease affects carbohydrate, fat, and protein metabolism and leads to progressive organ damage if not properly managed.
Definition of Diabetes Mellitus
Diabetes Mellitus is defined as a group of metabolic disorders characterized by chronic elevation of blood glucose levels resulting from absolute or relative deficiency of insulin and/or resistance to its action. Clinically, diabetes is diagnosed when fasting plasma glucose is ≥126 mg/dL, random plasma glucose is ≥200 mg/dL with symptoms, or HbA1c is ≥6.5%.
In simple terms, diabetes occurs when the body either fails to produce sufficient insulin or cannot effectively utilize the insulin produced, leading to impaired glucose utilization and persistent hyperglycemia.
Etiopathogenesis of Diabetes Mellitus
The development of diabetes involves a combination of genetic susceptibility, environmental triggers, and metabolic disturbances. The pathogenesis differs according to the type of diabetes.
Type 1 Diabetes Mellitus, the primary mechanism is autoimmune destruction of pancreatic β-cells in the islets of Langerhans, leading to absolute insulin deficiency. This autoimmune response is mediated by T-lymphocytes and is associated with autoantibodies such as anti-GAD antibodies. Genetic factors like HLA-DR3 and HLA-DR4 increase susceptibility, while environmental triggers such as viral infections may initiate the immune response.
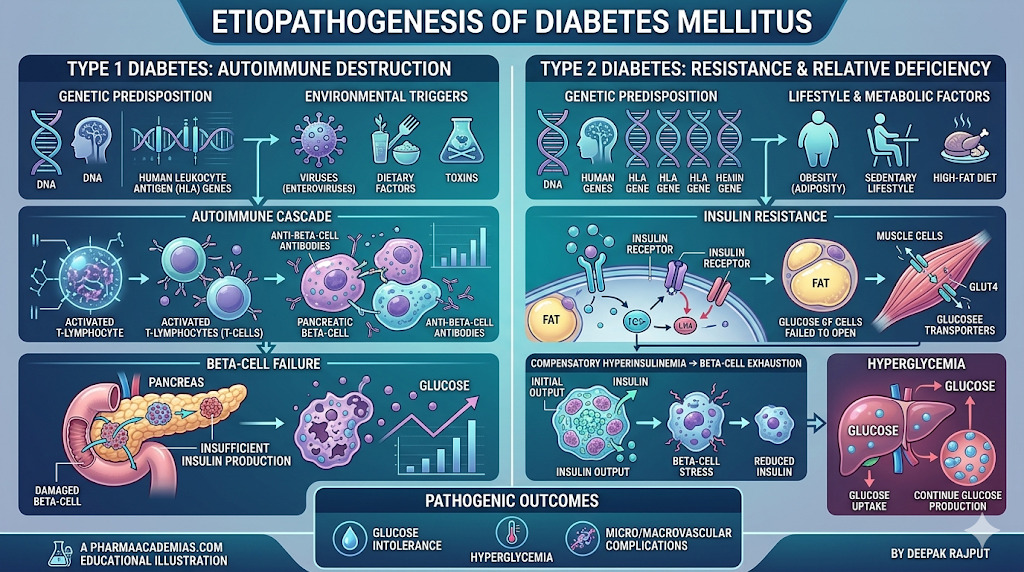
Type 2 Diabetes Mellitus, the central defect is insulin resistance in peripheral tissues, particularly skeletal muscle, liver, and adipose tissue, combined with progressive β-cell dysfunction. Obesity plays a crucial role by increasing free fatty acids and inflammatory cytokines such as TNF-α and IL-6, which impair insulin signaling. Initially, the pancreas compensates by increasing insulin secretion, but over time β-cell exhaustion leads to hyperglycemia.
Gestational diabetes develops during pregnancy due to placental hormones such as human placental lactogen, cortisol, and progesterone, which induce insulin resistance. When pancreatic compensation becomes inadequate, hyperglycemia occurs.
Other specific forms include genetic defects in insulin action, pancreatic diseases, endocrine disorders, and drug-induced diabetes.
Clinical Manifestations of Diabetes Mellitus
The clinical presentation depends on the severity and duration of hyperglycemia. Many patients with Type 2 diabetes remain asymptomatic in early stages and are diagnosed incidentally.
The classical symptoms include polyuria due to osmotic diuresis, polydipsia as a result of dehydration, and polyphagia due to cellular glucose starvation. Unexplained weight loss is more prominent in Type 1 diabetes due to fat and protein breakdown.
Patients may also present with fatigue, blurred vision, recurrent infections, and delayed wound healing. Infections of the skin, urinary tract, and genital region are common due to impaired immune function.
Long-standing diabetes leads to chronic complications affecting multiple organs. Microvascular complications include retinopathy, nephropathy, and neuropathy, while macrovascular complications include coronary artery disease, cerebrovascular disease, and peripheral arterial disease. Diabetic foot ulcers may develop due to neuropathy and poor blood circulation.
Acute complications include diabetic ketoacidosis, primarily in Type 1 diabetes, and hyperosmolar hyperglycemic state in Type 2 diabetes. Hypoglycemia may also occur as a complication of treatment.
Non-Pharmacological Management of Diabetes Mellitus
Non-pharmacological management is the foundation of diabetes care and is essential for all patients regardless of disease severity. Dietary modification plays a central role, emphasizing controlled carbohydrate intake, high fiber foods, and avoidance of refined sugars and saturated fats. Caloric restriction is important in overweight individuals to improve insulin sensitivity.
Regular physical activity enhances glucose uptake by muscles and improves insulin sensitivity. Moderate aerobic exercise combined with resistance training is recommended for optimal glycemic control. Weight reduction significantly improves metabolic parameters, especially in Type 2 diabetes.
Lifestyle modification also includes smoking cessation, limiting alcohol intake, stress management, and ensuring adequate sleep. Patient education regarding blood glucose monitoring, foot care, and adherence to therapy is essential for long-term disease control.
Pharmacological Management of Diabetes Mellitus
When lifestyle modifications are insufficient, pharmacological therapy becomes necessary.
Insulin therapy is essential in Type 1 diabetes and is also used in advanced Type 2 diabetes. Various insulin preparations include rapid-acting, short-acting, intermediate-acting, and long-acting formulations, which help mimic physiological insulin secretion.
Oral antidiabetic drugs are primarily used in Type 2 diabetes. Metformin is the first-line drug as it reduces hepatic glucose production and improves insulin sensitivity without causing weight gain. Sulfonylureas stimulate insulin secretion but may cause hypoglycemia. Meglitinides act similarly but have a shorter duration of action.
Thiazolidinediones improve insulin sensitivity through PPAR-γ activation but may cause weight gain and fluid retention. Alpha-glucosidase inhibitors delay carbohydrate absorption and reduce postprandial glucose spikes. DPP-4 inhibitors enhance incretin action, while SGLT2 inhibitors increase urinary glucose excretion and provide cardiovascular benefits. GLP-1 receptor agonists improve insulin secretion and promote weight loss.
In many cases, combination therapy is required to achieve optimal glycemic control. Acute complications such as diabetic ketoacidosis and hyperosmolar states require emergency treatment with insulin, fluids, and electrolyte correction, while hypoglycemia is managed with glucose administration.
Conclusion
Diabetes Mellitus is a complex chronic disease involving metabolic, genetic, and environmental factors. Its pathogenesis differs between Type 1 and Type 2 diabetes but ultimately results in hyperglycemia and multisystem complications. Early diagnosis, lifestyle modification, and appropriate pharmacological treatment are essential to prevent complications and improve quality of life. Effective diabetes management requires a comprehensive and individualized approach combining diet, exercise, education, and medications.


One Comment