Antihypertensive drugs are medications used to reduce elevated blood pressure and maintain it within the normal therapeutic range, thereby lowering the risk of complications such as stroke, myocardial infarction, heart failure, chronic kidney disease, and retinopathy. Hypertension is one of the most important modifiable cardiovascular risk factors worldwide, and effective pharmacological control significantly reduces morbidity and mortality. Current guidelines commonly target <140/90 mmHg for many adults, with lower individualized targets in diabetes, CKD, or high-risk cardiovascular disease.
These drugs work by reducing one or more of the following:
- cardiac output
- peripheral vascular resistance
- circulating blood volume
- sympathetic nervous system activity
- renin–angiotensin–aldosterone system (RAAS) activity
The overall aim is long-term protection of the heart, brain, kidneys, and blood vessels.
Classification of Antihypertensive drugs
Antihypertensive drugs are classified according to their site and mechanism of action.
The major classes include diuretics, beta-blockers, ACE inhibitors, angiotensin receptor blockers (ARBs), calcium channel blockers, alpha-blockers, central alpha agonists, direct vasodilators, and renin inhibitors. These remain the core therapeutic groups in modern antihypertensive therapy.
1) Diuretics
Diuretics lower blood pressure by promoting sodium and water excretion, thereby reducing plasma volume and cardiac output. With chronic use, they also reduce peripheral vascular resistance.
Thiazide diuretics such as hydrochlorothiazide and chlorthalidone are considered first-line agents in uncomplicated hypertension.
Loop diuretics, including furosemide and bumetanide, are especially useful when hypertension is associated with heart failure, renal impairment, or edema.
Potassium-sparing diuretics, such as spironolactone and amiloride, are valuable in resistant hypertension and hyperaldosteronism.
The major adverse effects include hypokalemia, hyponatremia, dehydration, hyperuricemia, hyperglycemia, and in spironolactone, gynecomastia and hyperkalemia.
2) Beta-Blockers
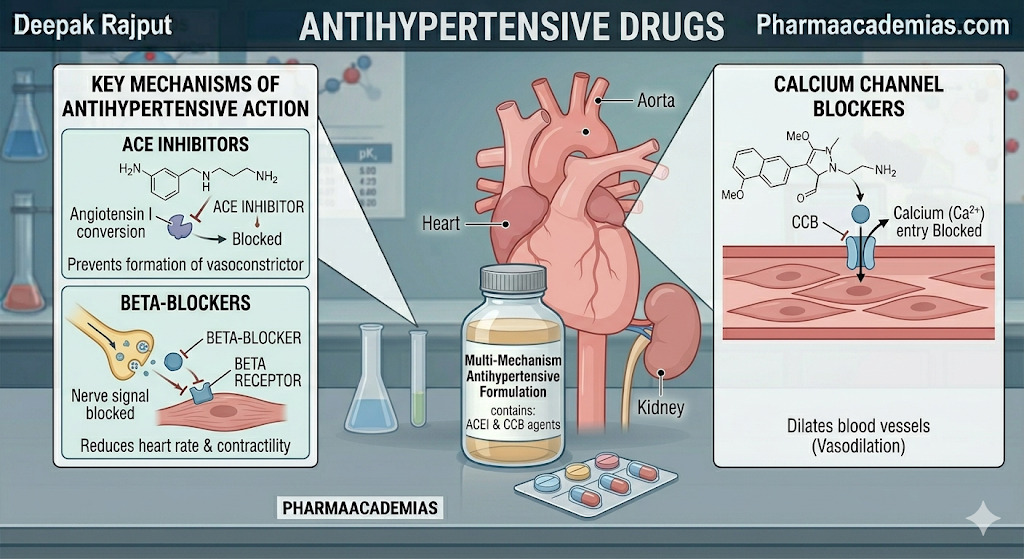
Beta-blockers reduce blood pressure by blocking beta-adrenergic receptors, which decreases heart rate, myocardial contractility, and renin release from the kidneys.
Common examples include metoprolol, atenolol, propranolol, bisoprolol, and carvedilol.
They are particularly useful in patients with:
- hypertension with angina
- post-myocardial infarction
- arrhythmias
- heart failure
- hyperadrenergic states
Common side effects include bradycardia, fatigue, bronchospasm, depression, cold extremities, and sexual dysfunction. They should be used cautiously in asthma.
3) ACE Inhibitors
ACE inhibitors block the conversion of angiotensin I to angiotensin II, leading to vasodilation, reduced aldosterone secretion, and decreased sodium retention. They also increase bradykinin, which contributes to vasodilation.
Important examples are enalapril, lisinopril, ramipril, and captopril.
They are preferred in:
- hypertension with diabetes
- diabetic nephropathy
- heart failure
- post-MI patients
- chronic kidney disease
Important adverse effects include dry cough, hyperkalemia, angioedema, hypotension, and renal dysfunction, especially in renal artery stenosis.
4) Angiotensin II Receptor Blockers (ARBs)
ARBs selectively block AT1 receptors, preventing the vasoconstrictor and aldosterone-secreting effects of angiotensin II.
Examples include losartan, valsartan, telmisartan, candesartan, and irbesartan.
Their uses are similar to ACE inhibitors, especially in patients who develop ACE inhibitor-induced cough.
Major side effects include hyperkalemia, dizziness, hypotension, and renal impairment.
5) Calcium Channel Blockers (CCBs)
CCBs reduce blood pressure by blocking L-type calcium channels, leading to vascular smooth muscle relaxation and vasodilation.
Dihydropyridines
Examples: amlodipine, nifedipine, felodipine
These mainly act on blood vessels and are excellent for isolated systolic hypertension and elderly patients.
Side effects include ankle edema, flushing, headache, and reflex tachycardia.
Non-Dihydropyridines
Examples: verapamil and diltiazem
These reduce heart rate, contractility, and AV conduction, making them useful in hypertension with arrhythmias.
Adverse effects include bradycardia, AV block, constipation, and worsening heart failure.
6) Alpha-Blockers
Alpha-1 blockers cause arteriolar and venous vasodilation, thereby reducing peripheral vascular resistance.
Examples include prazosin, terazosin, and doxazosin.
These are particularly useful in patients who also have benign prostatic hyperplasia (BPH).
The main side effects are postural hypotension, dizziness, palpitations, and first-dose syncope.
7) Central Alpha Agonists
These drugs stimulate central alpha-2 receptors, reducing sympathetic outflow from the brain.
Examples include clonidine and methyldopa.
Methyldopa is especially important in pregnancy-induced hypertension, making it a favorite exam question.
Adverse effects include sedation, dry mouth, constipation, and rebound hypertension on sudden withdrawal, especially with clonidine.
8) Direct Vasodilators
These drugs act directly on vascular smooth muscle to produce arteriolar relaxation.
Examples:
- Hydralazine
- Minoxidil
They are mainly used in severe or resistant hypertension.
Important adverse effects include reflex tachycardia, fluid retention, headache, lupus-like syndrome (hydralazine), and hirsutism (minoxidil).
9) Renin Inhibitors
The only major renin inhibitor is aliskiren, which directly blocks renin and suppresses RAAS activation at its initial step.
It is used in hypertension but less commonly than ACE inhibitors or ARBs.
Side effects include hyperkalemia, diarrhea, hypotension, and renal dysfunction.
Mechanism of Action of Antihypertensive drugs
The major antihypertensive mechanisms can be summarized physiologically as:
- Reduction of blood volume → diuretics
- Reduction of cardiac output → beta-blockers, non-DHP CCBs
- Vasodilation → ACE inhibitors, ARBs, CCBs, alpha blockers, vasodilators
- Suppression of sympathetic activity → beta-blockers, clonidine, methyldopa
- RAAS inhibition → ACE inhibitors, ARBs, aliskiren
Since BP = Cardiac Output × Peripheral Vascular Resistance, all antihypertensive drugs ultimately reduce one or both of these variables.
Uses of Antihypertensive drugs
These drugs are used not only for primary hypertension but also in several cardiovascular and renal disorders.
They are highly beneficial in: essential hypertension, secondary hypertension, chronic kidney disease, heart failure, post-myocardial infarction, diabetic nephropathy, hypertensive emergencies, and pregnancy-induced hypertension.
Drug selection depends on comorbidities:
- ACE inhibitors/ARBs → diabetes + CKD
- beta-blockers → post-MI + angina
- CCBs → elderly + isolated systolic HTN
- spironolactone → resistant hypertension
Side Effects of Antihypertensive drugs
The side effects vary by class but commonly include:
Electrolyte imbalance, especially with diuretics
Bradycardia and heart block with beta-blockers and verapamil
Dry cough and angioedema with ACE inhibitors
Peripheral edema with amlodipine
Orthostatic hypotension with alpha blockers
Sedation and rebound hypertension with clonidine
Hyperkalemia with ACE inhibitors, ARBs, spironolactone, and aliskiren
These adverse effects must be considered when individualizing therapy.
Conclusion
Antihypertensive drugs are one of the most important classes in cardiovascular pharmacology. They help reduce blood pressure, prevent end-organ damage, improve survival, and reduce cardiovascular events. Understanding their classification, mechanism of action, therapeutic uses, and adverse effects is essential for rational and safe prescribing.