Anti-ulcer drugs are a class of medications used to treat, prevent, and manage peptic ulcer disease and other acid-related gastrointestinal disorders. These drugs act by reducing gastric acid secretion, neutralizing existing stomach acid, protecting the gastric mucosa, or eliminating causative organisms such as Helicobacter pylori. They are among the most frequently prescribed drugs in medicine because disorders like gastric ulcer, duodenal ulcer, GERD, gastritis, and NSAID-induced ulceration are highly prevalent worldwide.
Peptic ulcers develop when there is an imbalance between aggressive factors—such as hydrochloric acid, pepsin, NSAIDs, and H. pylori—and defensive factors, including mucus, bicarbonate, prostaglandins, and mucosal blood flow. Anti-ulcer therapy is therefore aimed at restoring this balance and promoting mucosal healing.
Classification of Anti Ulcer Drugs
Anti-ulcer drugs are classified according to their mechanism of action and therapeutic target in gastric acid physiology.
1) Proton Pump Inhibitors (PPIs)
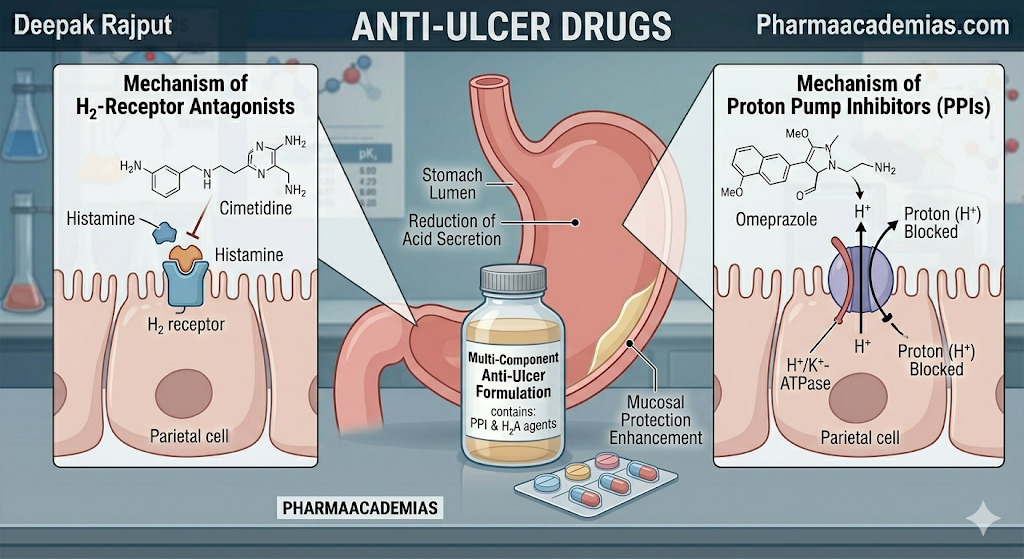
Proton pump inhibitors are the most effective anti-ulcer agents for long-term acid suppression. They act by irreversibly inhibiting the H+/K+ ATPase enzyme system (proton pump) in gastric parietal cells, which is the final step in acid secretion. This results in profound and long-lasting reduction of gastric acid production, allowing ulcers to heal rapidly.
Common examples include omeprazole, pantoprazole, esomeprazole, lansoprazole, and rabeprazole. These drugs are considered first-line therapy for peptic ulcer disease, reflux esophagitis, and Zollinger–Ellison syndrome.
2) H2 Receptor Antagonists
These drugs block histamine H2 receptors on gastric parietal cells, thereby reducing basal and stimulated acid secretion. Although slightly less potent than PPIs, they remain useful for mild to moderate acid-peptic disorders.
Examples include famotidine, cimetidine, and nizatidine.
A modern clinical note: ranitidine is no longer commonly recommended in many countries because of safety-related market withdrawal, so current practice favors famotidine as the preferred H2 blocker.
3) Antacids
Antacids provide rapid symptomatic relief by directly neutralizing gastric hydrochloric acid. They are especially useful in heartburn, dyspepsia, hyperacidity, and occasional acid reflux symptoms.
Common examples are magnesium hydroxide, aluminum hydroxide, calcium carbonate, and sodium bicarbonate.
4) Mucosal Protective Agents
These drugs protect the ulcer base and gastric lining from acid, pepsin, and bile salts. They form a physical barrier over the ulcer crater, promoting healing without significantly altering gastric acid secretion.
Important examples include sucralfate and bismuth compounds. Sucralfate is especially effective in duodenal ulcers, while bismuth is commonly used in H. pylori eradication regimens.
5) Prostaglandin Analogues
These agents mimic endogenous prostaglandins, especially PGE1, which help maintain gastric mucosal defense by increasing mucus and bicarbonate secretion and reducing acid output.
The most important example is misoprostol, which is particularly useful for the prevention of NSAID-induced gastric ulcers.
6) Antibiotics for H. pylori
Since Helicobacter pylori infection is a major cause of peptic ulcer disease, antibiotics are essential for eradication therapy.
Commonly used antibiotics include amoxicillin, clarithromycin, metronidazole, tetracycline, and tinidazole, usually given in combination with a PPI and sometimes bismuth.
Pharmacological Actions / Uses of Anti Ulcer Drugs
The pharmacological action of anti-ulcer drugs depends on their class, but their overall purpose is to promote ulcer healing, relieve symptoms, prevent recurrence, and reduce complications such as bleeding or perforation.
PPIs and H2 blockers mainly suppress gastric acid secretion.
Antacids neutralize already secreted acid.
Sucralfate and bismuth protect damaged mucosa and accelerate repair.
Misoprostol enhances mucosal defense and blood flow.
Antibiotics eliminate H. pylori, thereby treating the root cause of recurrent ulcers.
Dose of Anti Ulcer Drugs
The dose varies according to the specific drug, severity of disease, and treatment indication.
For example, omeprazole is commonly prescribed as 20–40 mg once daily, while pantoprazole is often given as 40 mg once daily for gastric and duodenal ulcers.
Famotidine is frequently used at 20–40 mg daily, depending on whether treatment is for active ulcer or maintenance.
For mucosal protection, sucralfate is commonly given as 1 g four times daily before meals and at bedtime.
In H. pylori eradication, PPIs are combined with two or more antibiotics for 10–14 days.
Dose adjustment may be required in:
- renal impairment
- elderly patients
- severe liver disease
- long-term therapy
Because long-term use, especially of PPIs, may cause adverse effects such as vitamin B12 deficiency, hypomagnesemia, fracture risk, and rebound hyperacidity, therapy should be individualized.
Indications of Anti Ulcer Drugs
Anti-ulcer drugs are indicated in a wide range of gastrointestinal conditions.
Their major indications include gastric ulcer, duodenal ulcer, peptic ulcer disease, gastroesophageal reflux disease (GERD), gastritis, Zollinger–Ellison syndrome, stress ulcer prophylaxis in ICU patients, and prevention of NSAID-induced ulcers.
They are also essential in H. pylori eradication therapy, where a PPI-based regimen forms the standard treatment.
In hospital settings, these drugs are often used to prevent stress-related mucosal bleeding in critically ill patients.
Contraindications of Anti Ulcer Drugs
Contraindications depend on the class of drug, but several important precautions apply.
Patients with known hypersensitivity or allergy to PPIs, H2 blockers, or other anti-ulcer agents should avoid their use.
In pregnancy, drugs such as misoprostol are strictly contraindicated because they can stimulate uterine contractions and may cause abortion. This is a very important exam point.
Patients with severe renal failure should use magnesium-containing antacids and sucralfate cautiously because of the risk of accumulation.
In liver dysfunction, dose adjustment may be necessary for drugs extensively metabolized by the liver, such as PPIs.
Drug interactions are another major contraindication concern. For example:
Cimetidine may inhibit hepatic enzymes and interact with warfarin, phenytoin, theophylline, and diazepam.
Long-term unnecessary PPI use should also be avoided in patients at risk of:
- osteoporosis
- recurrent C. difficile infection
- chronic kidney disease
- severe micronutrient deficiency
Conclusion
Anti-ulcer drugs are essential medications in the treatment of acid-peptic disorders and ulcer disease. Their main therapeutic actions include acid suppression, acid neutralization, mucosal protection, prostaglandin replacement, and bacterial eradication.
The major classes include proton pump inhibitors, H2 receptor antagonists, antacids, mucosal protective agents, prostaglandin analogues, and anti-H. pylori antibiotics. Proper understanding of their classification, uses, dose, indications, and contraindications is crucial for safe prescribing and effective ulcer management.