Anti-hyperlipidemic drugs, also known as lipid-lowering agents, are medications used to reduce elevated levels of cholesterol, triglycerides, low-density lipoprotein (LDL), and other atherogenic lipoproteins in the blood. Hyperlipidemia is one of the most important modifiable risk factors for atherosclerosis, coronary artery disease, stroke, peripheral arterial disease, and myocardial infarction. Persistent elevation of LDL cholesterol promotes plaque formation in arterial walls, leading to narrowing and hardening of blood vessels.
The main therapeutic goals of anti-hyperlipidemic treatment are to lower LDL cholesterol, reduce triglycerides, improve HDL cholesterol when appropriate, slow the progression of atherosclerosis, and reduce cardiovascular morbidity and mortality. Modern therapy is highly individualized based on lipid profile, cardiovascular risk, diabetes status, and presence of familial lipid disorders.
Classification of Anti-Hyperlipidemic Drugs
Anti-hyperlipidemic drugs are classified according to the pathway of lipid metabolism they target.
The major drug classes include statins, bile acid sequestrants, cholesterol absorption inhibitors, fibrates, niacin, omega-3 fatty acids, PCSK9 inhibitors, and newer emerging lipid-lowering therapies. Among these, statins remain the first-line treatment for most patients with dyslipidemia and cardiovascular risk.
1) Statins (HMG-CoA Reductase Inhibitors)
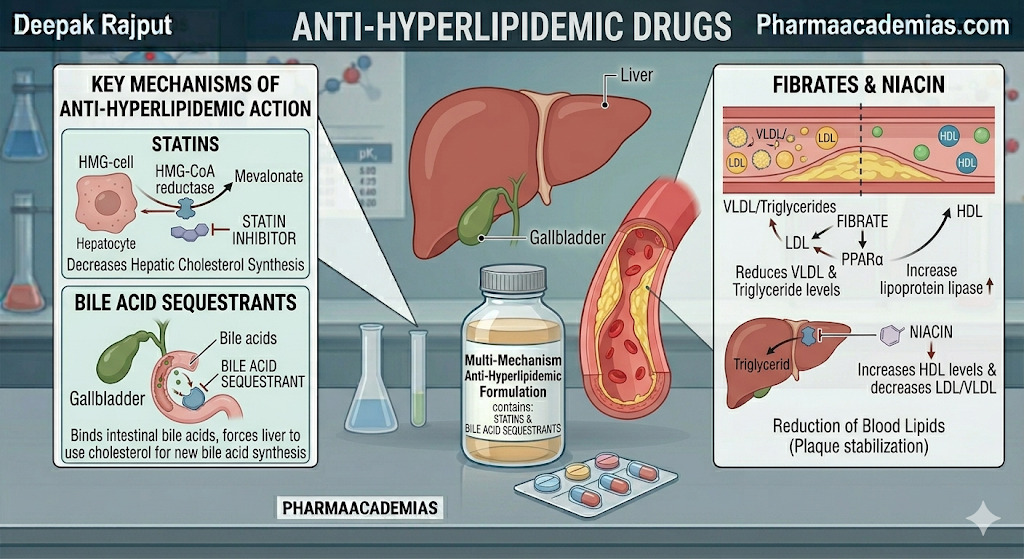
Statins are the most widely used and clinically important lipid-lowering drugs. They inhibit HMG-CoA reductase, the rate-limiting enzyme in hepatic cholesterol synthesis. As liver cholesterol synthesis decreases, hepatocytes respond by upregulating LDL receptors, which significantly increases the clearance of LDL cholesterol from the bloodstream.
Common examples include atorvastatin, rosuvastatin, simvastatin, pravastatin, and lovastatin.
These drugs are highly effective in:
- primary prevention of cardiovascular disease
- secondary prevention after myocardial infarction or stroke
- familial hypercholesterolemia
- mixed dyslipidemia
They can reduce LDL by up to 50–60% or more, depending on intensity.
2) Bile Acid Sequestrants
These agents bind bile acids in the intestine and prevent their reabsorption. Because bile acids are synthesized from cholesterol, this causes the liver to convert more cholesterol into bile acids, lowering plasma LDL levels.
Important examples include cholestyramine, colestipol, and colesevelam.
These are useful in:
- isolated hypercholesterolemia
- statin intolerance
- pruritus in biliary obstruction
However, they may raise triglycerides in susceptible patients.
3) Cholesterol Absorption Inhibitors
The most important drug in this class is ezetimibe. It selectively blocks the NPC1L1 transporter in the intestinal brush border, reducing dietary and biliary cholesterol absorption.
This decreases cholesterol delivery to the liver and promotes upregulation of LDL receptors, lowering LDL levels further.
Ezetimibe is especially valuable:
- as add-on therapy with statins
- in statin intolerance
- in familial hypercholesterolemia
It usually lowers LDL by 15–25% and has excellent tolerability.
4) Fibrates
Fibrates primarily target hypertriglyceridemia. They activate PPAR-alpha receptors, increasing lipoprotein lipase activity and accelerating the breakdown of triglyceride-rich lipoproteins.
Examples include fenofibrate and gemfibrozil.
Their major effects include:
- significant triglyceride reduction
- modest HDL increase
- reduced risk of pancreatitis in severe hypertriglyceridemia
They are especially useful when triglycerides are markedly elevated.
5) Niacin (Nicotinic Acid)
Niacin decreases hepatic synthesis of VLDL, which secondarily lowers LDL and raises HDL. It also reduces lipolysis in adipose tissue.
Although historically important, its use has declined because of adverse effects and limited cardiovascular outcome benefit compared with newer therapies.
It may still be considered in:
- mixed dyslipidemia
- low HDL with high triglycerides
- selected resistant cases
6) Omega-3 Fatty Acids
Omega-3 fatty acids such as EPA and DHA reduce hepatic triglyceride synthesis and improve triglyceride clearance.
They are especially useful in:
- severe hypertriglyceridemia
- prevention of triglyceride-induced pancreatitis
- cardiovascular risk reduction in selected patients
Prescription-strength EPA products have shown cardiovascular benefits in specific high-risk populations.
7) PCSK9 Inhibitors
PCSK9 inhibitors are among the most advanced lipid-lowering drugs. These monoclonal antibodies inhibit PCSK9, a protein responsible for LDL receptor degradation.
By blocking PCSK9, more LDL receptors remain available on hepatocytes, leading to dramatic LDL clearance from blood.
Examples:
- Alirocumab
- Evolocumab
These are particularly useful in:
- familial hypercholesterolemia
- very high-risk ASCVD
- statin intolerance
- patients not reaching LDL goals on maximal statin therapy
They may reduce LDL by 50–60% beyond statins.
8) Emerging and Newer Therapies
Newer drugs are increasingly important in modern lipidology.
Bempedoic Acid
This drug inhibits ATP-citrate lyase, an enzyme upstream of HMG-CoA reductase, reducing hepatic cholesterol synthesis.
Lomitapide
Used mainly in homozygous familial hypercholesterolemia, it inhibits microsomal triglyceride transfer protein (MTP).
Mipomersen
An antisense oligonucleotide that blocks ApoB-100 synthesis, thereby reducing VLDL and LDL production.
These are mainly reserved for severe genetic dyslipidemias.
Mechanism of Action of Anti-Hyperlipidemic Drugs
The overall mechanisms can be understood based on which lipid fraction is being targeted.
Statins and bempedoic acid reduce hepatic cholesterol synthesis.
Ezetimibe reduces intestinal cholesterol absorption.
Bile acid sequestrants increase cholesterol conversion into bile acids.
Fibrates and omega-3 fatty acids mainly reduce triglyceride-rich lipoproteins.
PCSK9 inhibitors increase LDL receptor recycling and LDL clearance.
These mechanisms together help normalize the lipid profile and reduce atherosclerotic plaque progression.
Uses of Anti-Hyperlipidemic Drugs
These drugs are used in both primary prevention and secondary prevention of cardiovascular disease.
The major clinical uses include:
- hypercholesterolemia
- hypertriglyceridemia
- mixed dyslipidemia
- familial hypercholesterolemia
- prevention of myocardial infarction
- prevention of stroke
- reduction of ASCVD risk
- prevention of pancreatitis in severe triglyceride elevation
Statins remain first-line for most patients, while fibrates and omega-3s are preferred when triglycerides dominate.
Side Effects of Anti-Hyperlipidemic Drugs
Adverse effects vary by drug class.
Statins may cause myalgia, myopathy, rhabdomyolysis, elevated liver enzymes, and rarely new-onset diabetes.
Bile acid sequestrants commonly produce constipation, bloating, nausea, and reduced absorption of fat-soluble vitamins.
Fibrates may cause gallstones, dyspepsia, liver enzyme elevation, and increased myopathy risk when combined with statins.
Niacin is known for flushing, itching, hyperglycemia, hyperuricemia, and hepatotoxicity.
PCSK9 inhibitors are generally well tolerated, with injection site reactions and mild flu-like symptoms being most common.
Bempedoic acid may increase uric acid and gout risk, which is an important modern exam point.
Conclusion
Anti-hyperlipidemic drugs are essential in the prevention and management of atherosclerotic cardiovascular disease and metabolic lipid disorders. Their major therapeutic role is to reduce LDL cholesterol, lower triglycerides, stabilize plaque, and prevent cardiovascular events. Statins remain the cornerstone of therapy, while newer agents such as PCSK9 inhibitors, ezetimibe, and bempedoic acid provide powerful options for patients needing additional LDL reduction.
A clear understanding of their classification, mechanism, uses, and adverse effects is essential for safe and rational pharmacotherapy.