While the kidneys are the primary organ for drug elimination, a significant number of drugs and their metabolites are eliminated through non-renal routes. Non-renal excretion pathways are especially important for drugs that are highly protein-bound, lipophilic, or poorly water-soluble, and for patients with renal impairment, where renal clearance is compromised.
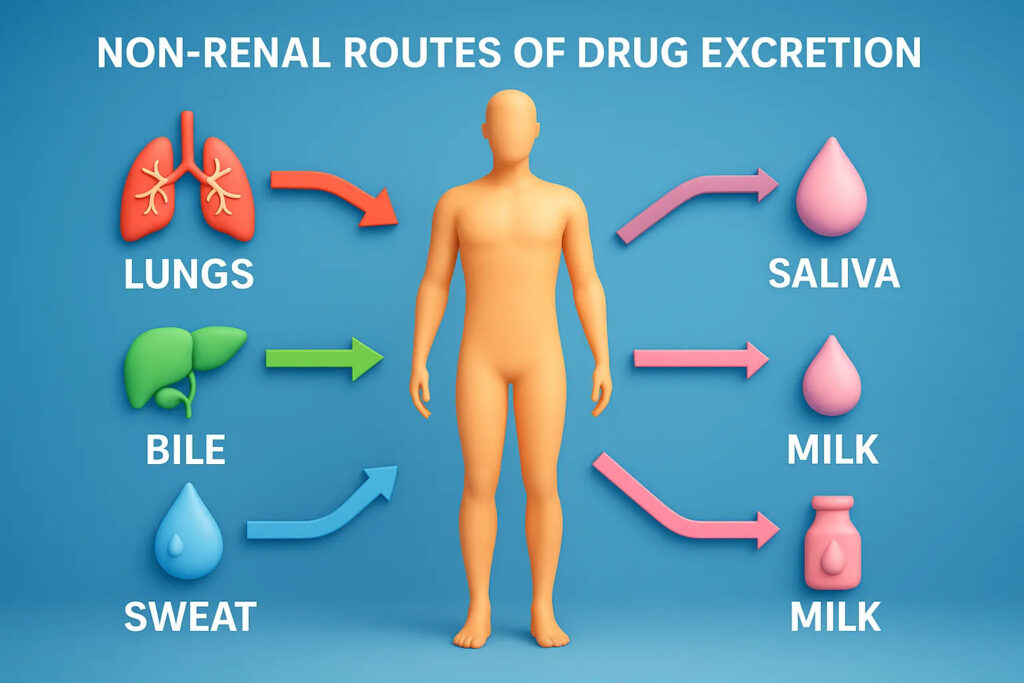
Non-renal excretion involves multiple organs and mechanisms, including biliary excretion, pulmonary excretion, sweat, saliva, milk, and gastrointestinal tract. Each route contributes to the overall pharmacokinetics and clinical effects of drugs.
1. Biliary (Hepatobiliary) Excretion
Biliary excretion is the major non-renal route for many drugs, especially those with high molecular weight (>500 Da), large polarity, and amphipathic properties. It involves secretion of drugs from hepatocytes into bile, which is then transported into the intestines and eliminated in feces.
Mechanism
- Drugs are taken up by hepatocytes via organic anion transporters (OATPs) or organic cation transporters (OCTs).
- Conjugation reactions (glucuronidation, sulfation, glutathione conjugation) often precede secretion, increasing water solubility.
- Bile flows into the small intestine, and drugs are excreted in feces.
- Some drugs undergo enterohepatic circulation, where bacterial enzymes hydrolyze conjugates in the gut, releasing free drug, which is reabsorbed.
Examples
- Morphine glucuronide – conjugated in liver → excreted in bile → reabsorbed partially
- Chloramphenicol glucuronide
- Erythromycin
- Digitoxin
- Bile acids and bilirubin conjugates
Clinical Relevance
- Drugs excreted in bile can be reabsorbed, prolonging their half-life.
- Obstruction of bile flow (cholestasis) can impair drug clearance.
- Some drugs undergo significant first-pass elimination via biliary excretion.
2. Pulmonary Excretion (Exhalation)
The lungs play a key role in eliminating volatile drugs and gases, primarily by diffusion from blood into alveolar air. This is most significant for volatile anesthetics and small gaseous molecules.
Mechanism
- Drugs diffuse along a partial pressure gradient from pulmonary capillaries into alveolar air.
- Clearance depends on:
- Blood solubility of the drug
- Pulmonary blood flow
- Ventilation rate
Examples
- Volatile anesthetics: halothane, isoflurane, sevoflurane
- Ethanol (small fraction)
- Nitrous oxide
- Gaseous poisons: carbon monoxide, hydrogen cyanide
Clinical Relevance
- Pulmonary excretion allows rapid elimination of anesthetic gases.
- Pulmonary diseases (emphysema, pneumonia) can impair clearance.
- Exhaled ethanol is the principle of breathalyzer tests.
3. Gastrointestinal (Fecal) Excretion
Some drugs are excreted directly into the intestines without hepatic involvement, or after biliary excretion. Drugs may also be unabsorbed orally and eliminated in feces.
Mechanism
- Passive diffusion into gut lumen (for poorly absorbed or lipophilic drugs)
- Active secretion via intestinal transporters
- Bacterial metabolism may inactivate or activate drugs
Examples
- Oral antibiotics: vancomycin, aminoglycosides (poorly absorbed → excreted unchanged)
- Cholestyramine-bound drugs (resins sequester drugs for fecal elimination)
- Digoxin (partly excreted via bile/feces)
Clinical Relevance
- Important for patients with renal failure, as fecal excretion may compensate partially.
- Alteration of gut flora may affect drug elimination (e.g., antibiotics disrupting enterohepatic circulation).
- Useful in treatment of overdose using adsorbents (activated charcoal, cholestyramine).
4. Sweat Excretion
A minor route of elimination, sweat contains water-soluble drugs that are excreted in small amounts.
Mechanism
- Passive diffusion of hydrophilic drugs into sweat glands.
- Lipid-soluble drugs are poorly excreted via sweat.
Examples
- Salicylates
- Lithium
- Heavy metals (lead, arsenic)
- Small amounts of some antibiotics
Clinical Relevance
- Generally negligible for therapeutic drug elimination.
- May contribute to dermal side effects or irritation (drug rash).
- Can serve as a non-invasive method for drug monitoring (e.g., sweat patches).
5. Saliva Excretion
Drugs can appear in saliva via passive diffusion, depending on their lipophilicity, ionization, and protein binding.
Mechanism
- Unionized, lipophilic drugs diffuse into salivary glands.
- The pH of saliva can influence ion trapping (similar to urine).
Examples
- Weak bases: amphetamines, caffeine
- Weak acids: aspirin
- Nicotine
Clinical Relevance
- Saliva sampling is used in therapeutic drug monitoring, drug abuse testing, and forensic analysis.
- Excretion is minor and does not significantly impact systemic drug levels.
6. Milk Excretion (Lactation)
Many drugs are excreted into breast milk, depending on molecular weight, lipid solubility, degree of ionization, and plasma protein binding.
Mechanism
- Passive diffusion into milk from maternal plasma
- Weak bases accumulate more in milk due to slightly acidic pH (pH ~7.0 in plasma vs 6.5–7.0 in milk → ion trapping)
Examples
- Weak bases: caffeine, codeine, morphine
- Alcohol
- Antibiotics: sulfonamides, tetracyclines
Clinical Relevance
- Can lead to neonatal drug exposure → toxicity risk
- Important consideration in breastfeeding mothers
- Some drugs (e.g., penicillin) are generally considered safe for infants due to low concentrations.
7. Minor Routes of Excretion
Other minor routes include:
- Hair and nails – accumulate drugs over time (used in forensic toxicology)
- Tears – very small amounts (e.g., pilocarpine, heavy metals)
- Cerumen (earwax) – negligible for systemic clearance
While clinically insignificant for therapeutic dosing, these routes are sometimes exploited in drug testing or forensic science.
Table of Non-Renal Excretion Routes
| Route | Mechanism | Examples | Clinical Relevance |
| Biliary/Fecal | Active secretion into bile, enterohepatic circulation | Morphine glucuronide, chloramphenicol | Important in liver disease, enterohepatic recirculation prolongs half-life |
| Pulmonary | Diffusion into alveoli | Volatile anesthetics, ethanol | Rapid elimination of inhaled drugs, breathalyzer tests |
| Gastrointestinal (direct) | Poorly absorbed oral drugs, passive diffusion | Vancomycin, aminoglycosides | Alternative in renal failure, overdose management |
| Sweat | Passive diffusion | Salicylates, lithium | Minor, may cause skin side effects |
| Saliva | Passive diffusion | Caffeine, amphetamines | Non-invasive monitoring, forensic use |
| Milk | Passive diffusion, ion trapping | Caffeine, codeine, morphine | Important in lactation, neonatal exposure |
| Minor (hair, nails, tears) | Accumulation | Heavy metals, drugs of abuse | Forensic toxicology |
Conclusion
Non-renal routes of drug excretion are essential complementary pathways for eliminating drugs, particularly for lipophilic, protein-bound, or hepatically metabolized compounds, and in patients with impaired renal function. Biliary excretion and pulmonary excretion are the most significant non-renal pathways, while sweat, saliva, and milk play minor but clinically important roles in therapeutic monitoring, toxicity, and neonatal safety. Knowledge of these pathways is crucial for dose adjustment, drug safety, and understanding pharmacokinetics.